Back to the Future: Why birth in the future will look more like birth in the past
- Lisa Baker
- Jul 13, 2019
- 7 min read
Updated: Jul 17, 2019
For much of Canada’s history, Indigenous and immigrant women gave birth in their homes or communities, usually surrounded by family members and assisted by a midwife (Relyea, 1992). Midwives were respected members of their community and received training formally or informally through a lifetime of experience and mentoring. By the end of the 19th century physicians began attending more and more births, first in family homes, and then in maternity wards of community hospitals. Midwives were still utilized in rural and remote communities and supported by the Government of Canada with the publication of a midwifery care guide (Relyea, 1992). However, most births were taking place in medical facilities by the mid 1900’s (The Vanier Institute of the Family, 2017). The number of midwifery-led births remained low into the 21st century, mainly because provincial and territorial governments did not legally recognize or fund midwifery-led birth until the late 1900’s (Mah, 2013). Today midwives attend about 10% of births in Canada (Canadian Association of Midwives (CAM), n.d.a).
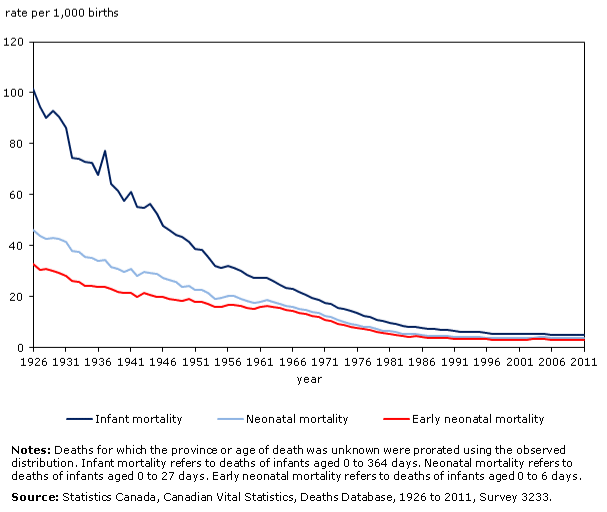
In the last 150 years, the number of medical interventions offered during birth has increased significantly. For the most part, this has been a positive improvement for maternity care. Figure 1 shows that the introduction of certain medical interventions significantly reduced maternal mortality rates in the 20th century (Institute of Medicine (US) Committee on Improving Birth Outcomes, 2003). Figure 2 shows similar trends for neonatal and infant mortality rates in Canada (Statistics Canada, 2015). Interventions such as cesarean sections, antibiotics, blood transfusions, aseptic techniques, and skilled care throughout pregnancy and birth have saved the lives of mothers and babies.

Paradoxically, continued increases in medical interventions during birth have not translated into improved birth outcomes for Canadian mothers and babies in the 21st century. This paradoxical relationship can be seen in the example of increasing cesarean section rates and increasing maternal mortality rates. There is no doubt that cesarean sections save lives. Careful introduction of cesarean section for select patients resulted in a decrease in maternal mortality rate in the first part of the 20th century (Low, 2009). But a cesarean section is an invasive surgery that comes with risks, including hemorrhage and infection. Overuse of cesarean section has been linked to increases in population rates of maternal depression, lower breastfeeding rates, and health complications in subsequent pregnancies (The Vanier Institute of the Family, 2015). To balance the benefits and risks of cesarean birth at a population level, the World Health Organization has calculated an optimal national cesarean birth rate of 10% (Betrán, Torloni, Zhang ,Gülmezoglu, & Zongo, 2015). When population cesarean birth rates rise higher than 10%, there is no additional reduction in maternal and neonatal mortality. There is, however, an increase in healthcare spending and an increase in poor maternal health outcomes (Association for Safe Alternatives in Childbirth (ASAC), 2016). In the past 25 years, Canada’s national cesarean birth rate has risen from 17.8% in 1994 to approximately 28% today (Health Canada, 2000; Public Health Agency of Canada, 2017). In this same time period, the number of maternal deaths in Canada has increased from approximately 4 deaths per 100,000 births in 1994 to somewhere between 5.1 and 11.9 deaths per 100,000 births today (Health Canada, 2000; Public Health Agency of Canada, 2017). These statistics suggest that an alarming number of mothers are experiencing unnecessary invasive surgery and are at a higher risk of poorer health outcomes. With each cesarean birth costing taxpayers almost 60% more than a home birth, these statistics also tell us we are spending a significant amount of money on medical interventions that are not always needed (ASAC, 2016). Why is Canada performing significantly more cesarean births than is deemed optimal by the World Health Organization? The answer to this, in part, is the definition of health used by healthcare providers.
As described in my post on May 30, 2019, the current definition of health as created by the World Health Organization needs transformation (Baker, May 30, 2019). However, it is within the confines of this classic definition of health that the medical model of birth has come to rest. In the medical model, birth is viewed as a medical condition that must be carefully monitored and treated (Our Bodies Our Selves, 2014). This type of model includes frequent use of medical interventions to assist the birthing process. Contrast this model with the physiological model of birth, as adopted by midwives throughout the world. In the physiological model, birth is viewed as a normal, healthy process that women can achieve with their bodies (CAM, n.d.b). These differing philosophies help to explain the differences we observe in the cesarean birth rates for women in general (29% in Alberta) and for women under the care of a midwife (7% in Alberta) (ASAC, 2016). Midwives achieve these low rates of cesarean birth for their clients without an increase in maternal and infant mortality (CAM, 2019). In fact, in their newly reaffirmed position statement on home birth, the Canadian Association of Midwives states that “the best available international evidence from jurisdictions where home birth services are integrated into the health care system demonstrates that midwife-attended, planned home births are associated with optimal labour and birth outcomes” (CAM, 2019).
Across Canada small maternity units have been closing due to rising healthcare costs and physician shortages in rural areas (The Vanier Institute of the Family, 2015). As already discussed, midwifery-led home births can help address rising healthcare costs and physician shortages. Yet, the amount of midwifery-led home births has not increased enough to compensate for the closure of small maternity units. Rather, many women are travelling great distances to give birth in larger cities, away from their families and communities. This disparity in maternity care is most pronounced for rural Indigenous families and has been reviewed in my post on July 2, 2019 (Baker, July 2, 2019).
Moving all births back into homes across Canada is not the way of the future. But if our healthcare system fully adopts the physiological model of birth, then many more births can take place at home, under the guidance of a professional midwife, safely and economically. I believe that maternity care of the future will place a larger emphasis on the use of technology and interprofessional collaboration (IPC) to deliver maternity care closer to home for as long as possible. Interprofessional teams will include families, nurses, midwives, physicians, other professionals as need. Mothers will play an active role in the monitoring of their own health closer to home and will be guided by the most appropriate care provider as her health needs dictate. In most cases, the midwife would be the most appropriate care provider, consulting with the physician as needed. In high-risk cases the physician or obstetrician would be the most appropriate care provider, consulting with the midwife and other professionals as needed. I describe this type of collaborative leadership in more detail in my May 24, 2019 post (Baker, May 24, 2019). A great amount of work has already been done to make this future vision of birth come to fruition in Canada. Pilot projects such as the HOPE app in Alberta and the OB Nest at the Mayo Clinic highlight the active role mothers can play in monitoring their own health needs from their own homes with the use of on-demand technology (Women and Children’s Health Research Institute, 2019; de Mooij et al., 2018). The Public Health Agency of Canada is in the process of releasing nine chapters of evidence-based recommendations in a set of national guidelines for family-centered maternity and newborn care. The principles used to shape the national guidelines affirm that birth is a normal, physiological process; that care close to home as possible is ideal; and that collaboration is key to family-centered care (Public Health Agency of Canada, 2018). Finally, midwifery associations across the country are working to increase access to midwifery care for all Canadians (CAM, 2018). With all of this exceptional work taking place, I believe birth in Canada is heading back to the future as it brings pregnancy, birth, and postpartum care closer to home for as many families as possible.
References
Association for Safe Alternatives in Childbirth. (2016). Maternity Care in Alberta. Retrieved from https://www.asac.ab.ca/wp-ontent/uploads/2018/01/Maternity_Care_in_Alberta_Report.pdf
Baker, L. (May 30, 2019). Defining health in the twenty-first century. Retrieved from https://lisabakerlcce.wixsite.com/eportfolio/post/defining-health-in-the-twenty-first-century
Baker, L. (May 24, 2019). Life lessons in interprofessional collaboration. Retrieved from https://lisabakerlcce.wixsite.com/eportfolio/post/life-lessons-in-interprofessional-collaboration
Baker, L. (July 2, 2019). Why are more Indigenous babies dying and what are we doing about it? Retrieved from https://lisabakerlcce.wixsite.com/eportfolio/post/why-are-more-indigenous-babies-dying-and-what-are-we-doing-about-it
Betrán, A., Torloni, M., Zhang, J., Gülmezoglu, A., & Zongo, A. (2015). WHO Statement on Caesarean Section Rates. BJOG: An International Journal of Obstetrics & Gynaecology. 123(5) doi: 10.1111/1471-0528.13526.
Canadian Association of Midwives. (n.d.a). Midwifery-led births per province and territory. Retrieved from https://canadianmidwives.org/2018/08/08/midwifery-assisted-births/.
Canadian Association of Midwives. (n.d.b). Mission and Vision. Retrieved from https://canadianmidwives.org/mission-vision/
Canadian Association of Midwives. (2018). Midwifery care for all: Building the profession Annual Report 2017-2018. Retrieved from https://canadianmidwives.org/wp-content/uploads/2018/10/Annual-Report-2017-2018.pdf
Canadian Association of Midwives. (2019). Position Statement on Home Birth. Retrieved from https://canadianmidwives.org/wp-content/uploads/2019/03/CAM_HomeBirthPS_EN_20190328_FINAL.pdf
De Mooij, M.J.M. et al. (2018). OB Nest: Reimaging Low-Risk Maternity Care. Mayo Clinic Proceedings, 93(4), 458-466. doi: https://doi.org/10.1016/j.mayocp.2018.01.022
Health Canada. (2000). Canadian Perinatal Health Report. Retrieved from http://publications.gc.ca/collections/Collection/H49-142-2000E.pdf
Institute of Medicine (US) Committee on Improving Birth Outcomes. (2003). Improving Birth Outcomes: Meeting the Challenge in the Developing World. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK222105/
Low, J. (2009). Caesarean Section – Past and Present. Journal of the Obstetricians and Gynaecologists of Canada, 31(12), 1131-1136. doi: https://doi.org/10.1016/S1701-2163(16)34373-0
Mah, C. L. (2013). Midwifery in Canada. LawNow. Retrieved from https://www.lawnow.org/midwifery-canada/
Our Bodies Our Selves. (2014). Models of Maternity Care. Retrieved from https://www.ourbodiesourselves.org/book-excerpts/health-article/models-of-maternity-care/
Public Health Agency of Canada. (2017). Perinatal Health Indicators for Canada 2017: A Report from the Canadian Perinatal Surveillance System. Retrieved from http://publications.gc.ca/collections/collection_2018/aspc-phac/HP7-1-2017-eng.pdf
Public Health Agency of Canada. (2018). Family-Centred Maternity and Newborn Care: National Guidelines. Retrieved from https://www.canada.ca/en/public-health/services/maternity-newborn-care-guidelines.html
Relyea, M.J. (1992). The rebirth of midwifery in Canada: an historical perspective. Midwifery 8(4), 159-169. doi: https://doi.org/10.1016/S0266-6138(05)80002-6
Statistics Canada. (2015). Canadian Vital Statistics, Deaths Database, 1926 to 2011, Survey 3233. Retrieved from https://www150.statcan.gc.ca/n1/pub/91-209-x/2013001/article/11867/fig/fig6-eng.htm
The Vanier Institute of the Family. (2015). Modern Maternity Care in Canada. Retrieved from https://vanierinstitute.ca/modern-maternity-care-canada/
The Vanier Institute of the Family. (2017). In Context: Understanding Maternity Care in Canada. Retrieved from https://vanierinstitute.ca/context-understanding-maternity-care-canada/
Women and Children’s Health Research Institute. (2019). Mental health app offers hope for pregnant women in Alberta. Spring 2019 Newsletter. Retrieved from https://www.wchri.org/newsletter



Comments